

OPINION
By Dr Dhesi BR, Dr Adlan Suhami, Khairul Omar
Various responses have been launched by different countries since the onset of the COVID-19 pandemic in their bid to minimize its toll within the shortest time possible. The enemy is unseen and its true nature unknown leaving governments either throwing all resources possible albeit the kitchen sink towards this affect. Conversely are those who opt for a liberal approach minimally restraining and relying upon good public literacy and trusting self-regulatory social measures.
Benchmarking governmental responses which may vary in timing and stringency as exemplified by the Oxford COVID-19 Government Response Tracker (OxCGRT) attempts to provide insights on the impacts following various state interventions. Towards this end, we visit various state interventions in the betterment of our understanding of how we have fared in relation to others.
Performa of Different Countries
Our comparative analysis goes further three-fold by combining disease trends of respective nations, testing and their stringency index in our attempt to provide greater width and depth of the effectiveness of respective policies implemented.
Data for the number of confirmed cases and deaths in the following sections is obtained from John Hopkins Coronavirus Resource Centre while the number of tests performed is sourced from Our World in Data, a collaboration between University of Oxford Martin Programme on Global Development and the non-profit organization Global Change Data Lab.
Performa of Different Nations
South Korea
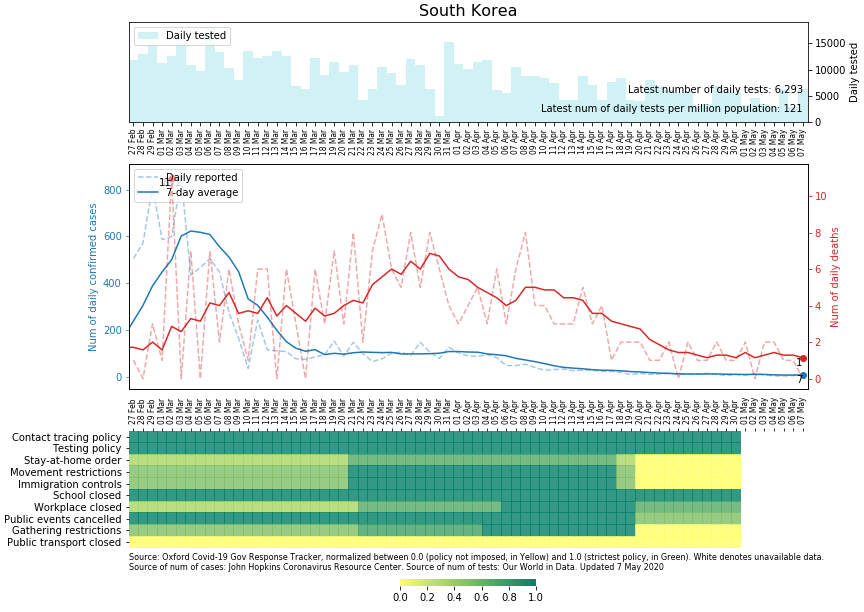
Table 1: Government Policies vs Cases
The number of daily cases was successfully brought to a stable base-line after an initial peak. Reciprocating was a steady increase in the number of fatalities as expected with a steady decline. South Korea had a consistent Testing Policy (TP) complemented by an automated Contact Tracing Policy(CTP) both of which, decisively instituted early and uninformedly. Apart from School Closure (SC) and Public Event Closure (PEC) South Korea eluded implementing stricter social measures vis lock-downs. Arguably, both policies of CTP and TP were pivotal in their success without resorting to stifling public movement nor to socio-economic activities.
Sweden
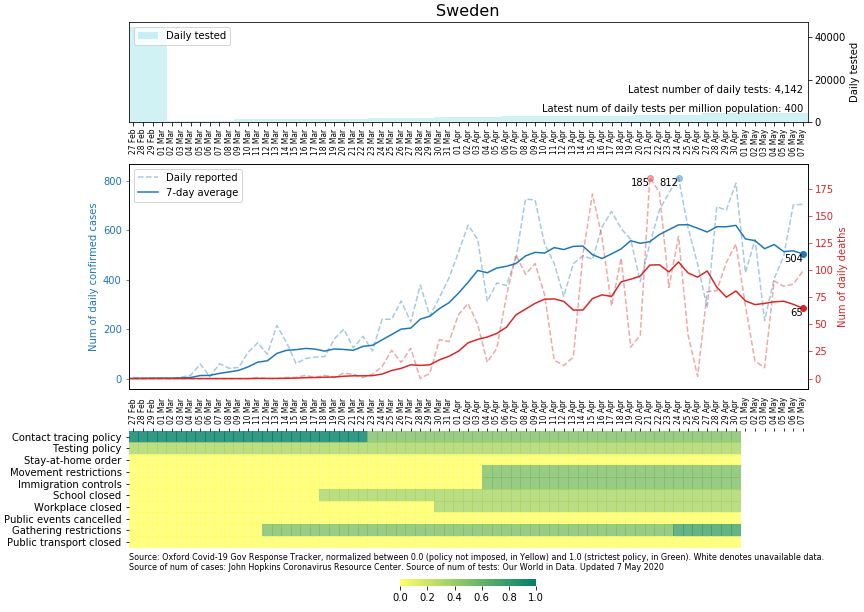
Table 2: Government Policies vs Cases
Sweden had from the onset opted for a sustainable policy. One which aims to attain Herd Immunity (HI) without overwhelming their healthcare services nor compromising the economy to much effect. Community suppression was avoided apart from school closure (kindergarten through grade nine were open). As with South Korea businesses, restaurants etc remained opened. Social distancing was self-imposed where many abided. Public literacy of the latter being an asset to their success as with in South Korea.
Tests were minimal as were other stringent social measures. Both number of cases and deaths (reaching 3000 cases to date) have steadily inclined. With a population of 10 million, Sweden leads other Nordic nations in the number of deaths. Their policy of waiting for natural immunity to develop remains which, largely is supported by the nation.
Singapore
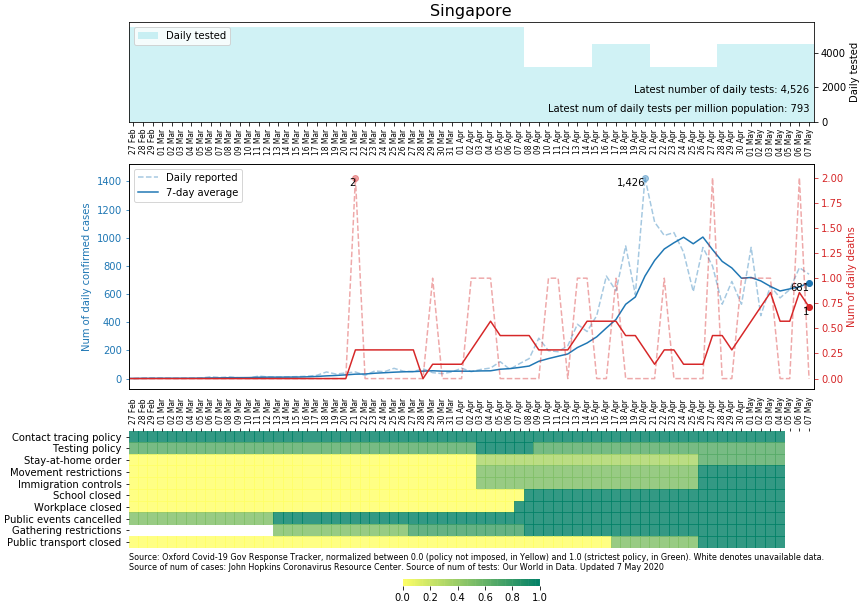
Table 3: Government Policies vs Cases
Singapore had extensive tests conducted from the onset. Similarly as with South Korea, automated CT played an important role in containing the outbreak at the initial phase, though compounded of late by local transmissions and by the foreign worker clusters. This is reflected by the late peaks of both cases and deaths of recent. Noteworthy is their early decision to practice wide-spread testing and stringent automated CTP allowing early detection and decisive informed intervention.
United Kingdom
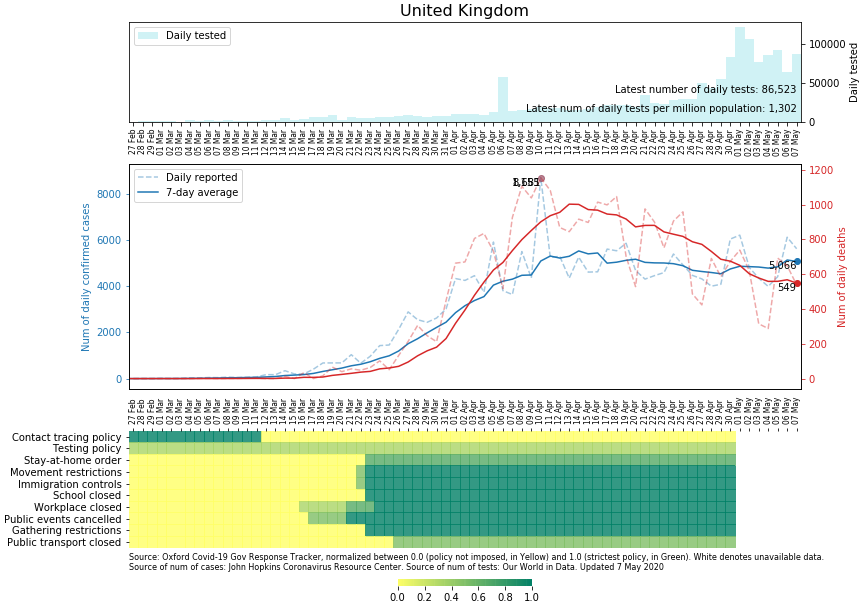
Table 4: Government Policies vs Cases
Initially opting for HI as with Sweden, the UK made a late decision to impose stringent policies vis lock-down and testing were ramped up in tandem. Clearly indecisiveness had resulted in the escalation of cases and with reciprocal deaths. The UK still continues to struggle with healthcare facilities being overwhelmed with the economy tail-gaiting in the aftermath.
Malaysia
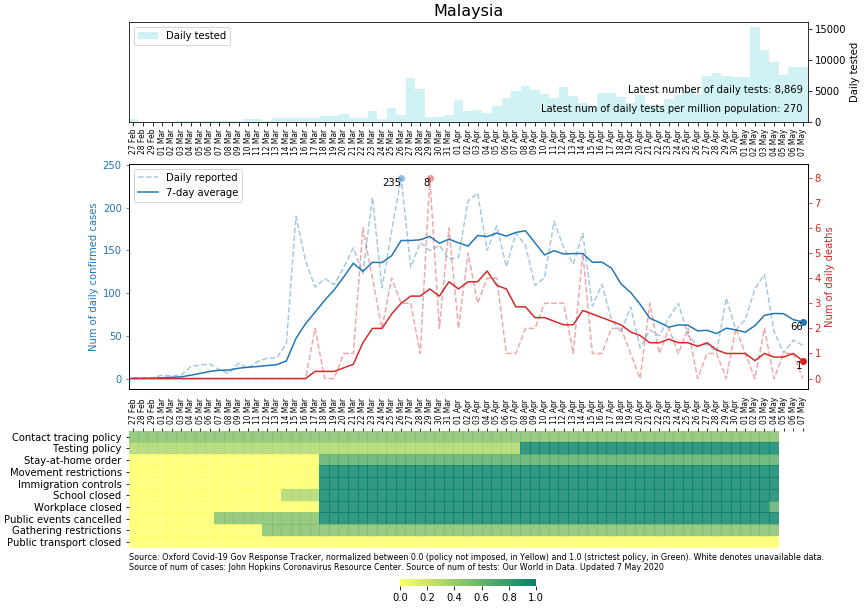
Table 5: Government Policies vs Cases
Strict public control measures were implemented in three phases from the onset. The number of official cases and deaths peaked gradually attaining an almost plateau-like crescendo with a decline following. Tests were incrementally instituted over time. Manual Contact Tracing is an on-going exercise in limiting the spread of the epidemic.
The government’s recent policy in gradually retracting the Movement Control Order (MCO) and its subsequent results will be much anticipated over time both on effects on health and on the social-economic front.
Matrix 1: Ranking of Stringency Index: Malaysia vs Western Countries
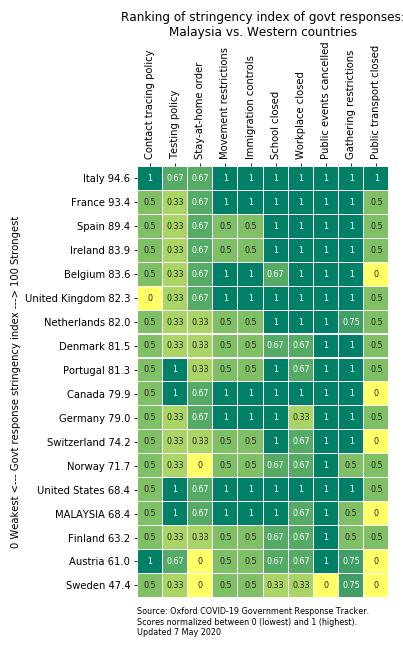
Malaysia was ranked at 68.4 on the Stringency Index ahead of developed nations such as Sweden and Austria. The total number of cases and deaths have been kept minimal throughout these measures.
Discussion
Various measures of stringencies have been instituted by different states in their efforts to contain the disease with different results. The outcome decided from the onset being crucial on the course of action being decided by different countries. Arguably many nations had opted for stringent measures as an immediate effect to prevent disease transmission and to reduce mortality. Some had decided for sustainability and had bitten-the-bullet to achieve Heard Immunity through community exposure at the expense of higher morbidity and mortality.
The role of Automated Contact Tracing has emerged as an important tool for early informed intervention, which is a hallmark of efficient outbreak management. Countries such as South Korea, Singapore and Taiwan have demonstrated that technology can effectively assist in outbreak management.
Big Data should be an essential tool of the future in this respect. It allows rapid data integration and analysis at the disposal of policy makers to execute important decisions. The dynamics of newly emerging diseases not only makes available valuable information for clinicians but also to policy makers and researches alike.
In this respect issues pertaining to greater data transparency, data confidentiality and data sharing is invaluable. The time has come to adopt a pragmatic approach towards data sharing especially in addressing global pandemics where the speed of communicating information affords early and pre-emptive action to be taken which, ultimately could save millions of lives.
Extensive testing with rapid Lab Turn Around Time (LTAT) has also shown to be pivotal in arresting chains of disease transmissions when implemented timely. Timeliness in attaining real-time-data as opposed to’ lag-time’ data allows not only one to assess the disease burden but also to allow early interventions. Dynamics of newly emerging diseases can also be analysed with the availability of timely data. Ultimately test results represent the most important variable which determines policy making.
The success of less stringent policies undertaken appear to be possible where communities had a high literacy on self-imposed social restrictions where, public compliance was crucial. It allowed society to function with almost normality albeit certain social restrictions. Socio-economic activities transpired with minimal stifling.
Various policies have been adopted by Malaysia with variable degrees of stringencies. Guided by the disease burden the outcome has been favourable to date. The decision to gradually lift social constraints was made to balance both health and non-health determinants. The next course of weeks will decide how effective these decisions are in sailing through the uncharted waters of the COVID-19 pandemic.
Conclusion
Benchmarking stringencies as a performa of favourable policies can serve as an important indicator in our quest to seek the best solutions. There is no ‘Magic Silver Bullet‘ policy to date rather comparisons of benchmarking to learn from. It should serve as a tool for continuous improvement on a journey to the finishing line of ending this pandemic.
Authors:
1. Dr Dhesi Baha Raja is a Public Health Medicine Specialist and Healthtech Advisor to the Former Health Minister of Malaysia. Award winner of the Pistoia Life Science King’s College London & MIT Top 10 Innovator Under 35.
2. Dr Adlan Suhami was the Former Deputy State Health Director of Sabah, Malaysia
3. Khairul Omar is a Senior Business Analyst who is currently based in the UK.
**All previous posts about COVID-19 here: https://sciencemediacentremalaysia.com/tag/covid-19/