

OPINION
By Dr Ng Siew Kit
At the initial stages of a new disease outbreak, information about the disease and how it spreads is scarce, limited and often incomplete. Therefore, it is difficult for the government and healthcare authorities to design management policies to contain the outbreak. To overcome this, scientists often rely on mathematical modelling to predict the future trend of a disease and consequently inform the appropriate measures to tackle the outbreak.
These models rely on the all-important “Re” value.
Re refers to the effective R(eproduction) number. In simple terms, it is the number of people an infected individual can infect at any given time. For example, if Re = 2, it means that every infected individual will infect another two individuals. Re determines whether a disease has the potential to develop into an epidemic or dies out naturally. If Re < 1, every round of infection leads to less victims, and there is no risk of an epidemic.

Trivia: Most people have heard about R0 as opposed to Re. R0 actually refers to the basic R(eproduction) number at time=0. This means the initial R-value at the beginning of a disease outbreak. As the outbreak progresses, the R-value may differ from the initial R0 due to different factors such conscious actions taken by humans, as well as viral mutations. Hence, the use of Re is more appropriate to describe an ongoing outbreak.
Epidemiological modelling can be extremely tedious as one must consider the many factors that govern the outcome of a disease outbreak. For the ease of explanation, we use SIR model to picture the general trend of a disease outbreak with direct human-human transmission (as in the case of COVID-19).
What is the SIR model?
In SIR models, individuals are separated into 3 groups, the Susceptible, the Infected, and the Recovered. The rate of change from susceptible to infected is denoted by transmission rate (β), and from infected to recovered by recovery rate (γ).

When generating a model, one must make assumptions. If these assumptions are met in the real world, the results of the model are likely to be accurate. In the modelling projection of COVID-19 below, the two important assumptions are that:
- 1. The infected individuals are infectious (i.e. can transmit the disease to others) throughout the period of infection.
- 2. The recovered individuals cannot be re-infected (i.e. are fully resistant to the disease).
Mathematically, in the SIR model:
The take-home concept from this formula is that the number of people infected by an infected person (Re) will fall when the recovery rate (γ) is faster ;but will rise when the transmission rate (β) and/or the fraction of the population susceptible to disease (S) increase.
Why do we need the MCO to control the COVID-19 epidemic?
The R0 value of COVID-19 is thought to be between 2 to 5. In order to control the COVID-19 epidemic in Malaysia, it is important that we bring down the Re value to less than 1 as soon as possible.
How can this be done?
1. Reduce transmission rate (β)
The mode of transmission of SARS-CoV-2 is mainly through aerosol droplets and surface contact. Whether this changes or not is reliant on viral mutations.
The chain of transmission can be broken by creating a barrier to protect uninfected individuals (wearing masks) and by reducing human contact (social distancing).
The MCO period has greatly increased social distancing and advocated for mask-wearing allowing the transmission rate to fall
2. Reduce the susceptible population (S)
This can be achieved naturally through “herd immunity”, where a significant proportion of the population develops immunity after recovering from the infection. However, this may overwhelm the healthcare system resulting in more deaths.
This can also be achieved through vaccination. However, a vaccine is currently unavailable.
3. Increase recovery rate (γ)
The infectious period can be reduced if infected individuals recover faster. Currently, there is no specific treatment for COVID-19.
Detecting and isolating infected individuals faster such that they no longer infect others. The current screening capability is insufficient.
Currently, for COVID-19, the only feasible option to rapidly reduce the Re value to ≤ 1 is to reduce the transmission rate through MCO-imposed social distancing. Despite it being difficult to reduce the susceptible population (S) and increase recovery rate (γ), the MCO essentially buys time for these options to mature. As other options mature (e.g development of drugs and vaccines, increased capacity of hospitals), the degree of restriction can be gradually relaxed.
Reducing transmission rate through MCO to flatten the curve
We can assume that Malaysia’s entire population of 32 million (S) is susceptible to COVID-19 initially. For modelling purposes, we will assume that the initial number of people infected (I) is 100 individuals and those infected take on average 14 days (0.07 years) to recover (γ).


At a high transmission rate (β), the infected population (I) in blue, spikes up quickly into a sharp peak. This means that there are many individuals infected during a short period of time. As shown, certain measures (i.e. social distancing, face masks, MCO implementation) can decrease the transmission rate. If such measures are successful, then we will “flatten” the blue infected population curve such that there will be less infected individuals at the peak of the curve, thereby protecting our healthcare system from being overwhelmed.
Decreasing Susceptible Individuals (S) through Mass Vaccination
Now let’s look at the likely effect of a mass vaccination programme designed to invoke immunity against SARS-CoV-2 (the virus that causes COVID-19). For COVID-19 modelling purposes, successfully vaccinated individuals are counted as “recovered”, as they are now resistant to SARS-CoV-2 infection. Let us also assume that I is still 100 individuals, the recovery rate γ is still 0.07 and that no measures to reduce transmission (e.g. MCO) are implemented (therefore transmission rate β does not change).
As you can see, vaccination programmes reduce the number of susceptible individuals (S) in a population. Even at a high transmission rate (β = 0.5), mass vaccination of more than 26 million of our population could drastically reduce the Re value and flatten the curve for up to a year.
Conditional MCO (CMCO)
Malaysians are well aware that our economy is suffering under MCO, and there is a need to maintain a delicate balance between our economy and COVID-19 management. Yet the implementation of the conditional MCO (CMCO) which started from 4th May 2020 was greeted with caution. Only time will tell whether such a move to bolster our economy is premature or not.
During the MCO period, our country has substantially increased our healthcare capacity both in terms of numbers and quality to handle COVID-19 cases. We are also increasing our capability to effectively screen for and isolate infected individuals in a shorter amount of time. Given that, we can hypothetically relax some of the movement restrictions necessary for resuscitating our economy through the CMCO which can also buy time to further improve these measures.
However, in my opinion, we will be dependent on global players for drugs and vaccine development against COVID-19, as our country is lacking in these aspects.
A quick look on how we have achieved the 6 criteria listed by WHO on guidelines for lifting lockdown restrictions:
1. Disease transmission is under control
2. Health systems are able to “detect, test, isolate and treat every case and trace every contact”
3. Hot spot risks are minimized in vulnerable places, such as nursing homes
4. Schools, workplaces and other essential places have established preventive measures
5. The risk of importing new cases “can be managed”
6. Communities are fully educated, engaged and empowered to live under a new normal
I believe we have met 1, 5, and are in the process of establishing robust 2, 3, 4. The real worry is actually 6. As a community, we reacted well in 6 during MCO, but we can begin to see signs of trespassing the new normal since CMCO.
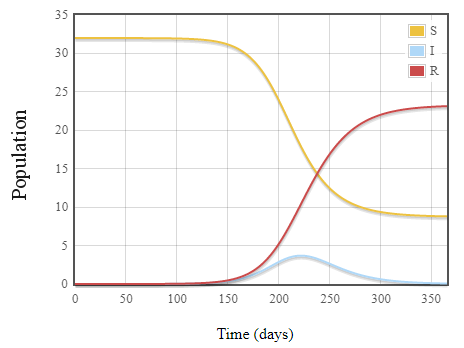
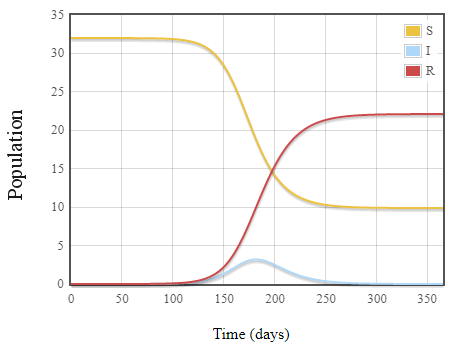
Maintaining the MCO Re value during CMCO
In this model, we assume that the transmission rate (β) of COVID-19 during the CMCO is between that of during the MCO and voluntary social distancing. We can also assume that our screening and isolation procedures are better now, therefore reducing the number of “infectious” days (i.e. recovery rate γ) of each individual on average. We will also assume that the number of infected individuals (I) in the community has already been halved at the time of the CMCO implementation.
Using these values, you can see that the COVID-19 epidemic projection is strikingly similar under both scenarios (MCO vs Conditional MCO).


Overall conclusion
Once again, it is important to note that some of the values used in this SIR modelling are not the exact numbers applicable to the COVID-19 epidemic in Malaysia. However, I hope that this modelling explanation can help clarify why the MCO was absolutely necessary from 18th of March onwards, as it was the only option on the table (i.e. reducing transmission rate β). Many steps have been taken towards reducing the Re to ≤ 1 during the MCO period.
Critically, Malaysians have to embrace the new norm aimed at suppressing the transmission rate (β) and increasing the “recovery” rate (γ) of COVID-19 moving forward. Remember, until vaccines are widely available, the COVID-19 outbreak can only be quenched when the transmission rate (β) is consistently lower than the “recovery” rate (γ).
Tip: As a rough guide, you can take a quick glance at the daily “New vs Recovered” case numbers.
Estimating the probability of an outbreak developing
By 18 March 2020, it was clear that there were SARS-CoV-2 spread within our community that cannot be holed up through aggressive contact tracing. This stochastic modelling tells us that if no actions were taken at that point, an epidemic will definitely break out. With the benefit of hindsight, the MCO declaration was in time (still 2-3 days late to allow for preparation, in my opinion) to prevent more widespread COVID-19 epidemic.
Using stochastic modelling, the probability (P) of an epidemic is:
P = 1-(1/Re)i0
where i0 = initial number of infected individuals
Re = basic reproduction number
The probability of an infectious disease developing into an outbreak is thus dependent on the Re value and the initial number of infected individuals (i0).
Most estimates of the R0 for COVID-19 lies between 2 and 3, and it is reasonable to assume that the R0 in Malaysia is somewhere within the similar range.
Example to demonstrate how different factors affect probability of outbreak
If Re = 2.5, and the number of initial infected individuals (i0) is just 5, the probability of an outbreak is ~ 99% !!
When Re = 1.5, the probability of an outbreak is ~86.8% if 5 individuals are initially infected. However, if the number of initial infected individuals (i0) are more than 11.4, with the same Re value, there is a 99% chance of an outbreak.
At Re = 1.1, there is a ~37.9% chance of an outbreak if 5 individuals are initially infected. The probability drops to ~31.7% if the initial number of infected individuals is 4, and less than 25% if only 3 are initially infected.
Using stochastic modelling, you can see that a lower Re can drastically reduce the probability (P) of an outbreak from happening. The number of initial infected individuals (i0) can also affect this probability.
Try the maths yourself:
If we managed to control the R0 to ≤ 1, there would be a 0% chance of an outbreak no matter what the initial number of infected individuals are!
Dr Ng Siew Kit is a senior lecturer at the Advanced Medical and Dental Institute, Universiti Sains Malaysia (AMDI, USM). He is also the principal investigator within the RNA-Bio Research Group at AMDI, USM with his main research interest on antiviral innate immunity.
* This is the personal opinion of the writer or publication and does not necessarily represent the views of Science Media Centre Malaysia
**All previous posts about COVID-19 here: https://sciencemediacentremalaysia.com/tag/covid-19/